SpiroConnect® Data Manager Software implementation
of the ATS/ERS 2019 Guidelines Update.

Standardization of Spirometry 2019 Update. An Official American Thoracic Society and European Respiratory Society Technical Statement1.
Key Updates
- A new list of relative contraindications was added.
- Spirometers are now required to meet International Organization for Standardization (ISO) 26782 standards, but with a maximum permissible accuracy error of ±2.5%.
- Device quality assurance procedures were updated.
- Operator training as well as attainment and maintenance of competency were addressed.
- The list of activities that patients should avoid before testing was updated.
- There is a focus on the use of devices that measure both expiration and inspiration.
- Maneuver acceptability and repeatability criteria were updated. The end of forced expiration (EOFE) was redefined.
- Requirements for spirometry systems to provide uniform cues and feedback to the operator were added.
- New withholding times for bronchodilators before bronchodilator responsiveness testing were developed.
- A new grading system for assessment of spirometry quality was developed.
- Standardized operator feedback options that promote synoptic reporting were developed.
- Preliminary findings derived from an international patient survey were presented.
MAJOR CHANGES:
Acceptability and Usability Criteria
The objective is to obtain the best result for the subject on the day of the test. Various aspects of the manoeuvre need to be considered in order to be sure the subject has achieved the very best result.
Failing to satisfy all these aspects does not necessarily invalidate the results completely but will mean that they will be a less reliable estimate of their true lung function. Rather than deleting all the data from unsatisfactory tests, it is better to retain these and then base the final results on the best tests obtained. A single unsatisfactory test result may still be able to answer a clinical question, for example whether the subject has sufficient function to be able to undergo a surgical procedure. If results are derived from tests that are in some aspects unsatisfactory, then the operator must draw attention to this fact in Examination Notes2.
SPIROCONNECT® DATA MANAGER SOFTWARE MAJOR CHANGES IMPLEMENTATION:
When the application is launched SpiroConnect® Data Manager Software (SDM) will automatically check for an updated software version if the PC is connected to the internet. If an updated version is available, the operator will be taken to a download page where he can download the installer for the newer version. This file should be downloaded and then run to complete the update.
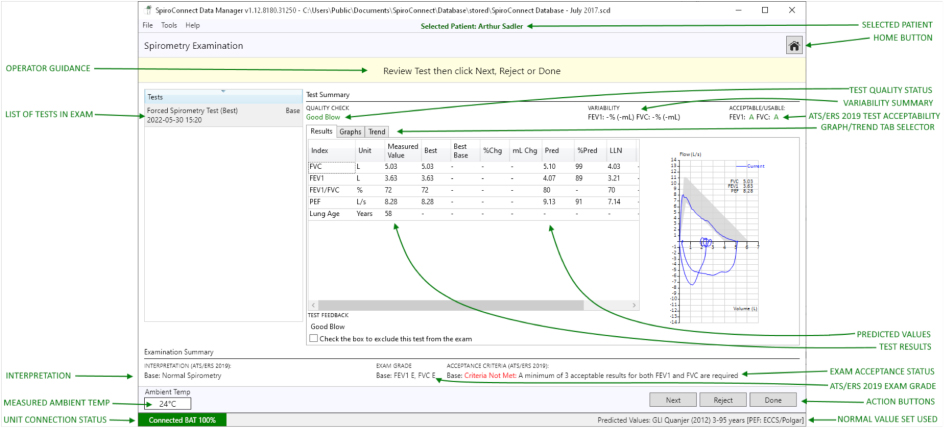
In the SpiroConnect® Data Manager software (SDM) the individual blow quality check message for the blow is displayed and could be one of the ten following messages: hesitant start, slow start, no plateau, hesitant at Max Vol, low volume, incomplete inspiration before expiration, low final inspiration, slow filling, cough in first second and good blow (further explanation and comments how to address these issues are detailed in the SpiroConnect® Spirometer Operators Manual Issue 1.12.1)
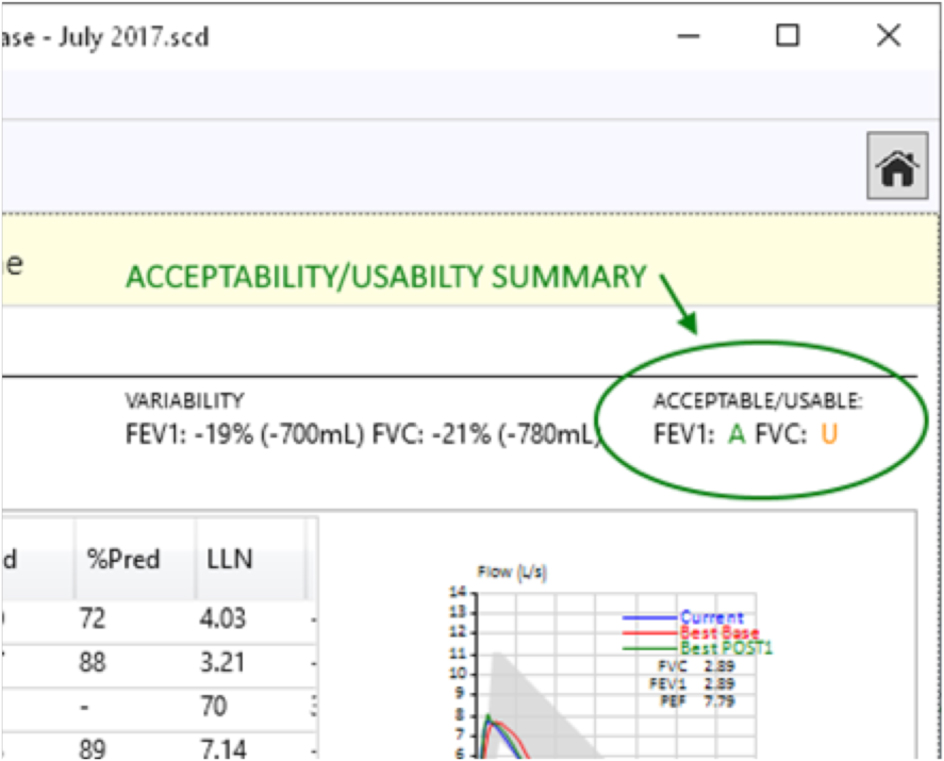
The SDM software automatically determines whether the FEV1 and FVC from each specific test should be used for interpretation or not, in accordance with rules published in the ATS/ERS 2019 update. Measurements of the FVC and FEV1 in each blow have been categorised as ACCEPTABLE (A), USABLE (U), or in case of NOT USABLE display would show: (-).
All parameters that have been selected for display in SDM Settings are shown, along with the predicted value (if available), best baseline value (*Base) and percentage change from Best Base blow (if the blow is a Post blow), blow quality assessment, ATS/ERS 2019 FEV1 and FVC acceptability status for this blow, ATS/ERS 2019 exam grade for the exam as a whole, overall examination quality assessment and interpretation. The values used for the interpretation are always the values in the 'Best' column. These values comprise the best results for each parameter, taken from all tests of acceptable quality from the current exam stage, in accordance with ATS/ERS guidelines.
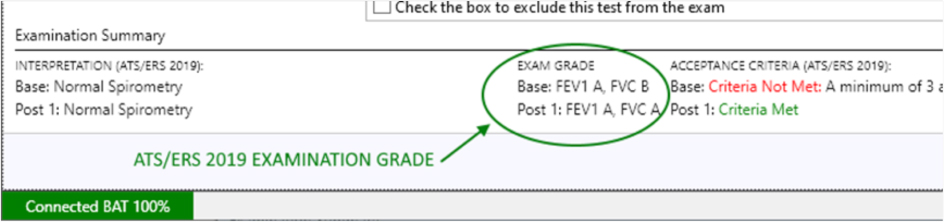
The ATS/ERS 2019 update also introduces the concept of Exam Grade. This is an overall grade that is given to an exam based upon how many FEV1 and FVCs were acceptable/usable/not usable and what the reproducibility between the best values was. The operator should always aim to get the highest exam grade possible. The grading system goes as follows (from best to worst): A, B, C, D, E, U, F (A-E Acceptable, U = Usable, F = Fail). To achieve the Exam Grade A three or more acceptable efforts are required with FVCs and FEV1s within 150 mL of each other (100 mL in children under 6). The Exam Grade is displayed on-screen in the Examination Summary section:
Grading System for FEV1 and FVC
| Grade | Number of Measurements | Repeatability Age >6yrs | Repeatability Age<6yrs |
| A | ≥3 acceptable | Within 0.150 L | Within 0.100 L |
| B | 2 acceptable | Within 0.150 L | Within 0.100 L |
| C | ≥2 acceptable | Within 0.200 L | Within 0.150 L |
| D | ≥2 acceptable | Within 0.250 L | Within 0.200 L |
| E | ≥2 acceptable or 1 acceptable |
>0.250 L N/A |
>0.200 L or 10% of the highest value, whichever is greater N/A |
| F | 0 acceptable and ≥1 usable | N/A | N/A |
| G | 0 acceptable and 0 usable | N/A | N/A |
ATS/ERS 2019 acceptance criteria1:
- At least 3 acceptable FEV1 and 3 acceptable FVC must exist within the exam stage
- The two largest FVC values must be within 150mL of each other, or for patients aged 6 or younger, 100mL or 10% of largest FVC, whichever is greater
- The two largest FEV1 values must be within 150mL of each other, or for patients aged 6 or younger, 100mL or 10% of largest FEV1, whichever is greater
- The two largest VC values must be within 150mL of each other or 10% VC (whichever is smaller) for patients older than 6 years; and 100mL or 10% of largest FVC, whichever is smaller (for patients aged 6 or younger)
Relaxed vital capacity
Measurements of RVC should always be recorded prior to a forced manoeuvre, because forced manoeuvres may induce bronchospasm/obstruction. It is best practice to perform an initial measurement of an RVC manoeuvre because relying on FVC measurements alone can lead to an underestimation of lung volumes in the elderly and those with dynamic airway collapse (eg, COPD, emphysema)2. It is important to remember that if in SDM forced spirometry is performed first, there will be no option to add a Relaxed Spirometry test.
End of forced expiration
The end of forced expiration occurs when the subject can blow out no more air and defines the VC. Premature termination of the blow will lead to an underestimate of the FVC and will falsely increase the FEV1/FVC ratio.
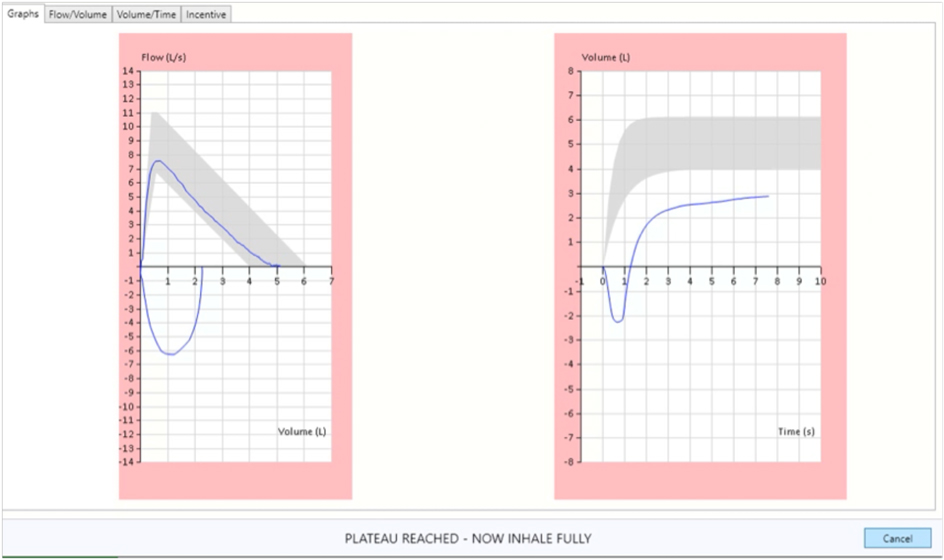
One of the indicators of the end of a forced expiration is a plateau on the Volume/Time graph with less than 0.025 L being expired over the last 1 s of the test. However, some subjects with severe airflow obstruction never achieve such a plateau even after exhaling for 20 s. Previously it has been suggested the blow should be maintained for at least 6 s in adults, but younger subjects may complete the manoeuvre in less time than this, as do patients with a severe restrictive defect2. The graph border will change to green when the duration of the exhalation passes 6 seconds
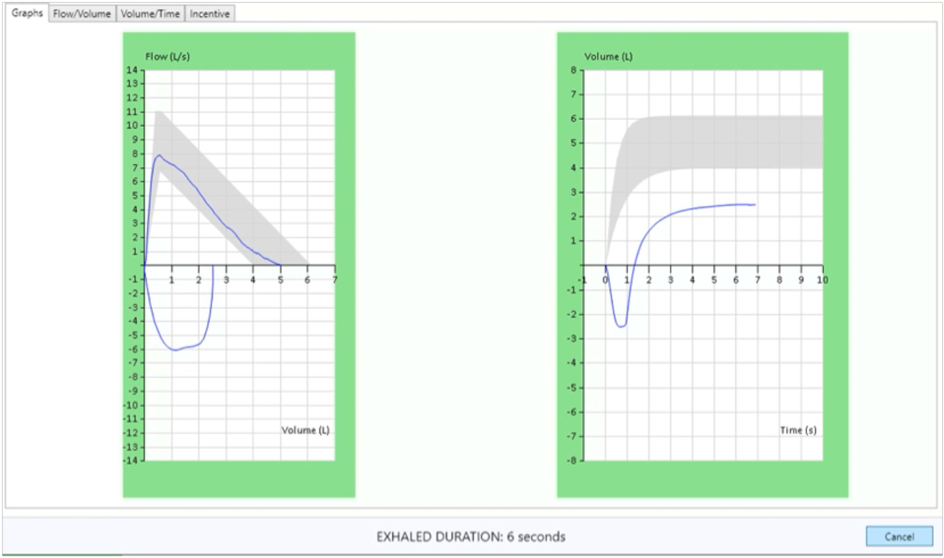
The operator should always encourage the subject to blow out for as long as possible. Failure to obtain a plateau and/or 6 s of exhalation is not ground to reject the blow. Exhalation times of >15 s are unlikely to change clinical decisions2. SDM software automatically detects the plateau and beeps once if it is reached in forced maneuvers and twice in relaxed manouvres. In addition, a pink border around the graphs will appear when a plateau is detected.
DETAILED SDM AND FIRMWARE CHANGES (not all changes are listed as we continuously work on our software development):
| V1.12 PC Software (SDM) changes: | V3.02 Firmware (SpiroConnect® Unit) changes: |
| Calibration routine made simpler with messaging changes Calibration low flow target change to 0.5 - 2LPS Force relaxed graph ticks to change to 5 sec if blow > 20 sec (only in live graphing) Trend graph on printed reports/PDF will now only go up until the date of the exam under Review Existing Exams Button Text Changed the option to automatically modify settings to those which are best for ATS/ERS 2019 compatibility Added warning if settings are not ideal for ATS2019 Post BD wait time < 15 mins warning added Additional post BD test > 15mins warning added Clear EXHALED DURATION text when results arrive Changed 'EV' to 'BEV' Changed Birth Gender to Birth Sex Removed ATS2005 from acceptance criteria Added mouseover tips for acceptance/usability and exam grade Changed Test Guidance to show 'exclude' and 'mark good' buttons but no quality feedback when in ATS 2005 mode Prevent Test Feedback from being shown in pre-ATS2019 exams Exam Notes feature general improvements Added standardised E11 operator comments addition to Exam Notes changed ARTP repeatability limits in line with 2020 advice PDF Print Preview window added Added Pack Years prompt in link mode Added Pack Years to Patient Data Added Ulna Length calculator as alternative to patient height Changed Low FVC warning box to a non-blocking type Added pack Years to Examination. Exam Patient table Include/Exclude right click functions added Apply FEV/FVC predicted values, z-Score, SDs to FEV1/VC in GLI Added warning for FEV1 dropping below 80% or prior best Added exam grade to printout, PDF reports Separated FEV1 and FVC acceptability summaries Improved colour coding for ATS quality messages Added quality overrides to settings Added Low Volume quality check Make ATS2019 the default acceptance criteria Make quality String Provider return different text depending on whether Exams are partially ATS2005 or completely ATS2019 Added MARK GOOD function to test feedback section Added quality guidance to test feedback section Added UNMARK GOOD ability with checkbox in feedback section Allow MARK GOOD/UNMARK GOOD at any point until DONE is clicked Added FEV1 + FVC Acceptability to Exam Review Make VT graphs start from point of max inhalation Changed calibration accuracy requirements to ±2.5% values Add Time To PEF, Prev MIF, Plateau Detected, Loop Start Time, Hesitation Time, Firmware Version, Unit SN to Forced Test Table, add Tidal Unstable, Plateau Detected, Firmware Version, Unit SN to Relaxed Test Table. Add Force Good Quality to Forced Test and Relaxed Test tables Add ATS 2005, ATS2019 reproducibility calculators Changed graph scaling to start at -1sec (VT graphs) Added feedback region on screen during live testing for exhaled duration and plateau Allow MARK AS GOOD function to work on any poor quality test in the current stage before the stage is ended |
Added PLATEAU DETECTED flag in relaxed spirometry Added 15 second timeout warning packet Large number of changes (added internal parameters) to support ATS/ERS 2019 compliant quality checks (such as hesitation time, mean inspiratory flow) Improvement to IRV, ERV calculation Change logic so that IC and ERV are always calculated unless relaxed test consists of a single inhalation or exhalation Only allow tidal calculation if the 3 tidal breaths volumes are within 30% Changed logic for VC calculation so it can never get skipped Add UNSTABLE_TIDAL flag Prevent inspiratory results before expiratory results are done - inspiratory results should always be for the loop following the expiratory loop Terminate SVC after 15 tidal cycles without stability Changed tidal variability req from 20% to 15% now signal TIDAL DONE when the % criteria is not met, but 10 breaths have passed Changed PEAK TIME to time from 10% - 90% of PEF (ATS2019) Changed PLATEAU beep in FORCED to single beep (ATS2019) Changed TIDAL MET beep to single beep (ATS2019) Changed PLATEAU beep in relaxed to double beep (ATS2019) Added 15 second expire time beep in forced, relaxed, both are a double beep (ATS2019) blow timeout changed to 4 seconds |
Brian L. Graham, Irene Steenbruggen, Martin R. Miller, Igor Z. Barjaktarevic , Brendan G. Cooper , Graham L. Hall , Teal S. Hallstrand , David A. Kaminsky , Kevin McCarthy , Meredith C. McCormack , Cristine E. Oropez , Margaret Rosenfeld , Sanja Stanojevic , Maureen P. Swanney , and Bruce R. Thompson ; on behalf of the American Thoracic Society and the European Respiratory Society.
Karl Peter Sylvester, Nigel Clayton, Ian Cliff, Michael Hepple, Adrian Kendrick, Jane Kirkby, Martin Miller, Alan Moore, Gerrard Francis Rafferty, Liam O'Reilly, Joanna Shakespeare, Laurie Smith, Trefor Watts, Martyn Bucknall and Keith Butterfield.